

Empowering Gynecologic Exams: Speculum Care Without Stirrups
Many thanks to all the University of Michigan midwifery students for letting me know that content and images from this post were shared in this week’s lectures! Re-posting for this week’s #tbt. Originally posted November 2016.
…
A couple of years ago I wrote a post entitled "12 Ways to Be A Feminist Healthcare Provider." In that post, I made a quick reference to the fact that I no longer use the foot pedals/stirrups during GYN exams. This includes including vaginitis checks, pap smears, bimanual exams, IUD insertions or removals, rule out rupture of membranes in triage, cervical exams in labor... you name it!There are a number of reasons I've ditched the stirrups for (almost all* of) my speculum exams.
Stirrups place people's legs and feet in a restricted position which inhibits free movement or a change in position due to pain or discomfort during the exam.
People with a history of sexual assault may be triggered by restricted movement during a gynecologic exam.
When people put their feet in the stirrups, it positions their pelvis downward, almost making it a requirement that their butt be slightly off the end of the exam table to improve access to the cervix: the feeling of falling off the table is also uncomfortable for many people, and may actually cause them to tense their pelvic floor to keep from falling, making the speculum exam painful.
Stirrups are technically unnecessary for exams: they make access easier for the provider, which isn't feminist/humanist care nor empowering care unless the provider cannot access the cervix by standard means and a position change might facilitate an accurate exam or more comfort for the patient.
Foot holders/stirrups generally aren't comfortable.
For some scripting related to the exam itself, check out the post on "Feminist Midwife Scripts: Painful Cervical Exams in Labor." All of my posts are meant to serve both people who seek healthcare and those who provide it, so please read and comment regardless of whether you are a provider or receiver of speculum exams!A number of people have expressed confusion about how exactly it works to not have room below the exam table for speculum maneuvers, citing concern that there isn't room for the speculum handle. Excellent question! Ditching all concern over holding a speculum outside of my pants in the name of showing some visuals, here is a pictorial guide featuring yours truly! (Many thanks to my Tuesday midwifery student for taking the pictures!)A few notes:
I use the word "patient" as it is both gender neutral and is common terminology in medical instruction care. I in no way mean to use this word as an indicator of power differential or as a dehumanizing term. Client, person, care-seeker, vagina-owner, cervix-owner... all take equal credence in my vocabulary, but here I stick with patient to make it consistent in its differentiation from "provider." Thanks for understanding.
Plastic speculums are what are used in my clinic. If you use metal / different sizes more regularly, compare your speculum handle size to the height difference between the exam table and the extended table.
Even if you are using stirrups, consider the fact that a change in the position of the speculum itself, rather than a change in the position of the patient, might facilitate a better view of the cervix. Try different positions of the speculum handle, including to the left or right side and upside down (while always maintaining posterior pressure as you would with the common position of the handle downward) to see if the cervix appears easily with speculum direction.
If you do not have exam tables that have an extender/mini table, try the same instructions below with the person positioned further up on the exam table and their feet on the same table: likely their pelvis will be pointed upward enough to complete an exam. Having them move their feet further toward their butt or putting a folded blanket under their hips can also help with upward pelvic tilt.
Some people will argue that making the foot pedals more comfortable can be an approach to making the exam more comfortable for people. Sure, perhaps that's true. My argument is that it is the restricted patient position in the holders themselves that usually only benefits the provider. Making a restricted position more comfortable is not the same as taking away the restrictions and finding comfort that way.
Regardless of this general argument toward stirrup-less exams, if you as the provider are more comfortable with stirrups and thus feel like you can provide a better exam and be empowering in other ways by minimizing speculum movement.
As always, in the comments here and on social media, please be mindful of gender pronouns, as gynecologic exams, those needing speculum care, and vagina-owners do not always identify in the binary or might but with varied pronouns. Be inclusive, y'all :)
Thoughts about certain kinds of exams:
IUD insertions: For IUD insertions, many people feel that stirrups provide a better position for long-term visualization during the procedure. Perhaps that is true for some people, as I, too, have encountered the speculum that wanders away from a cervix and outward during longer exams. In this circumstance, I find the extended table helpful because the handle will move outward and downward and be stopped by the table often before it comes out completely. Perhaps with the next IUD insertion, try the extended table, ask the patient to bear down and see if the speculum moves. If not, you should be good to continue with the extended table. If it moves away from the cervix or outward, there may need to be more support to maintain speculum position than just a change in patient position.
Speculum self-insertion: People for whom the speculum exam is a feared visit or is uncomfortable and the exam itself is absolutely necessary for their care, there are many things I do to try to increase comfort (send them home with a few speculums and lube to allow them time to practice at home and get used to it, for example). Another method is that they insert the speculum on their own (similar to how ultrasonographers offer people the opportunity to insert a trans-vaginal probe on their own). With stirrups as the default position, people are unable to navigate the body maneuvers (hands, torso, legs) needed to position oneself to insert the speculum and then lay down for the provider to complete the exam. The extended table allows this process to happen much more easily.

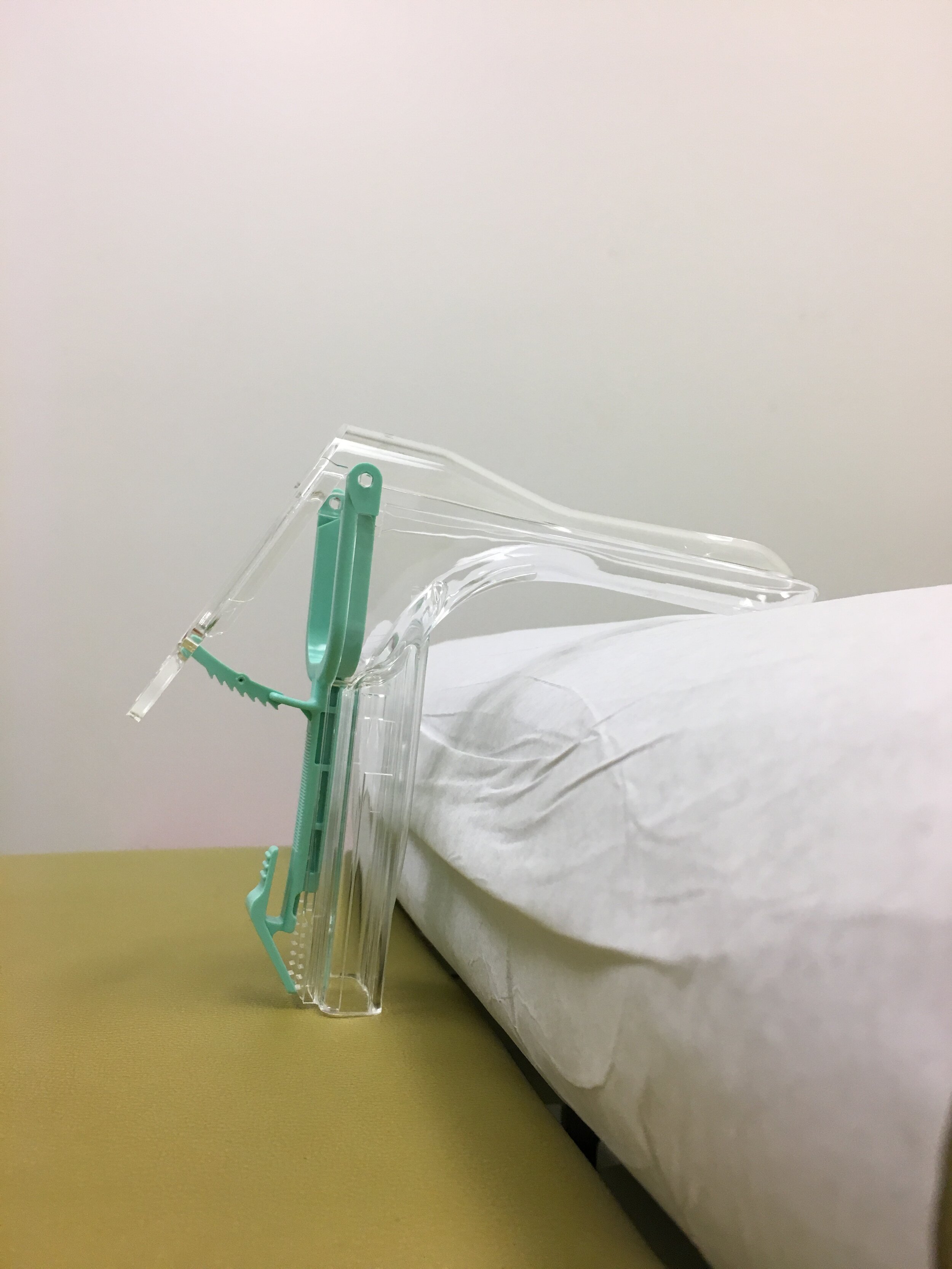





Picture #1: Try this in your own clinic - how much space is between the top table and the extended table? If it's at least a hand-width, try going stirrup-less!Pictures #2 and #3: Note that when the speculum handle encounters the extended table, there is no way that the end of the speculum would be visualizing the cervix at this point. This is to show that the handle interacting with the extended table is not an issue.Picture #4: Generally, I have the extended table pulled out completely, and people place their feet on the outermost corners. For many, just this position allows access for comfortable speculum care. Depending on the amount of inner leg tissue and vulvar tissue, I might ask people to drop their knees out to the sides if they can, or if they don't mind my moving the tissue with my hand(s).Pictures #5, #6, and #7: Here, I am demonstrating that with my feet on the extended table, my pelvis is tilted upward. Thus, when I hold the speculum at the entry point, the handle is well away from the extended table. (With stirrups, the legs are extended downward and thus the pelvis is too, which would cause the handle to bump into the table if both the stirrups and the extended table were present.)*For anyone who has a difficult time supporting the weight of their own legs or who has joint pain or difficulty bending / abducting / adducting, one or both stirrups may be more comfortable for their care. Chat with your patient about what makes them most comfortable during an exam, or what you could do to make it more comfortable for them, and include stirrups versus the extended table as part of the discussion.What are your experiences going stirrup-less? For providers, are there certain circumstances you've found this doesn't work well? For people who seek speculum care, would offering stirrup-less exams make a difference for you? What about self-insertion of the speculum?As always, I'm looking forward to the comments and discussion!- Stephanie